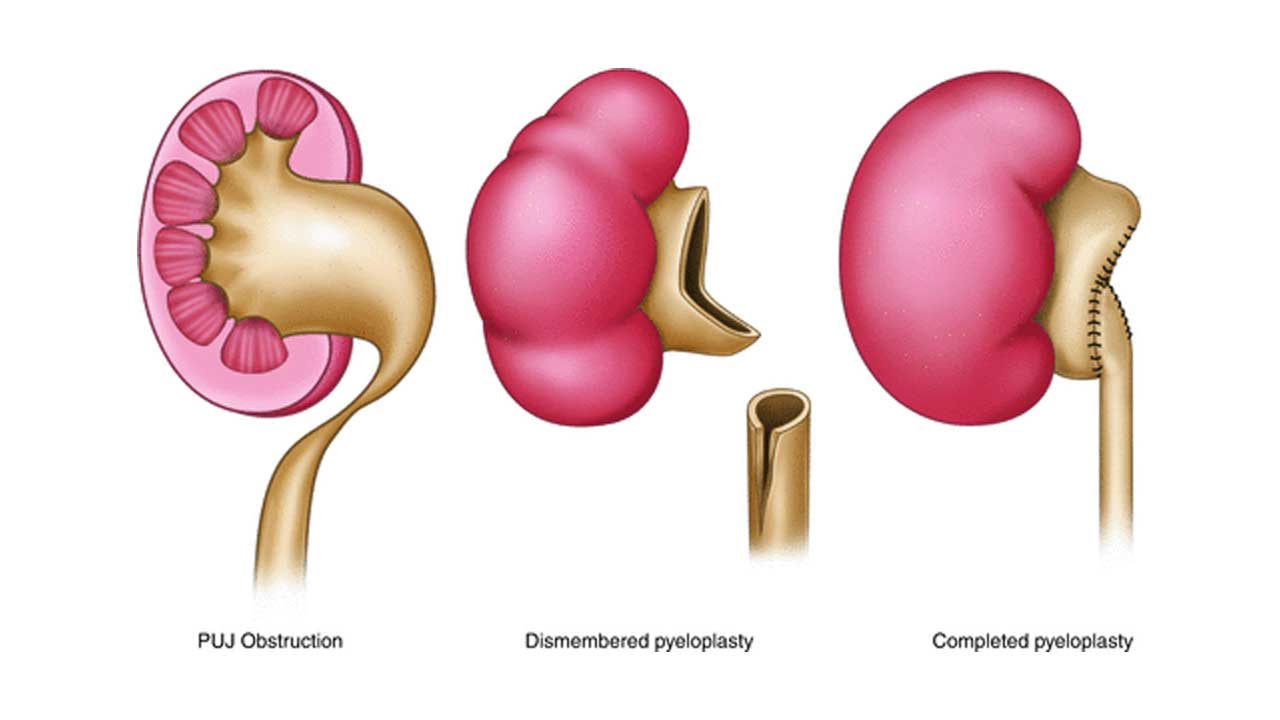
This is an operation to repair / reconstruct a narrowing between the pelvis of the kidney and ureter. Please read PUJ OBSTRUCTION – pt guide for further details about the condition.
I have been told that I need a pyeloplasty. What happens next?
It is likely that you would have already had some blood tests and scans. In addition, the anaesthetist will need to see your ECG and chest x-ray; and, in some, an echocardiogram (ultrasound scan of your heart) as well.
It is likely that your urologist has gone through the procedure in detail including the short, medium and long-term complications. You may have already signed the informed consent form for the operation. If this is not the case, it is likely to be obtained after admission to hospital.