It was 6 am. On the dot. I wake up, as is my routine, without the aid of an alarm clock. I have been doing so for the past 45 years. I am 64 now, a retired civil servant. I light the first of several cigarettes for the day and head to the toilet. With the pleasures of modern living, thankfully, we have a western wc. I start voiding into the pan, and felt something was not right. There is an odd sensation in my water passage during voiding. I look down and notice that I am peeing blood mixed with a few clots. Panic rising, I sit down on the toilet seat. I thought this was just an oddity, something that will pass. It did. The second void after my breakfast was less coloured and by mid-morning it was completely clear. I was vigilant for the next 48 hours, but there was no recurrence of the episode. I mentioned this to my wife who then insisted on a visit to our family doctor. This then led to a referral to a urologist, who gave me a clean bill of health after a few tests, but did quip, “I am sure this is a timely warning for you to quit smoking Mr Sharma!”

Blood in Urine
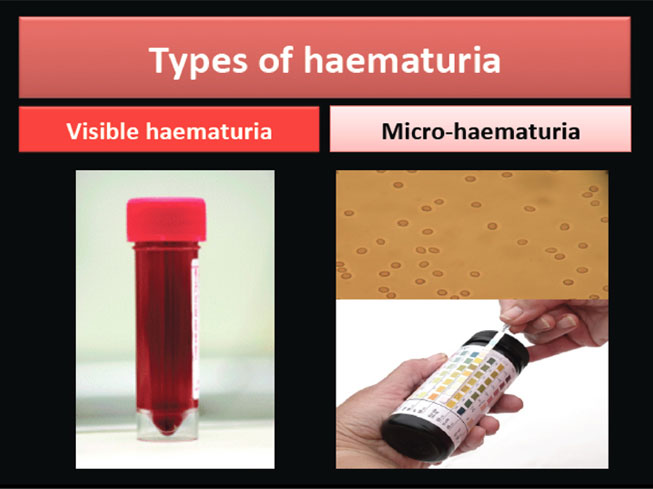
Blood in the urine (haematuria) can be an alarming symptom. Mr Sharma is one of those lucky individuals who have visible blood in the urine (visible haematuria) but with no significant cause found for it. About 60-70% of people with visible haematuria do not have any identifiable pathology, but the rest have significant disease or abnormality detected in the urinary tract. More importantly, up to 30% of this group may have an underlying malignancy in the urinary tract. In contradistinction to visible haematuria, blood identified on dipstick testing or microscopy of a urine sample (micro-haematuria), although still a concern, has far less ‘pick up’ of an ominous diagnosis; in mass screening programs the pick up rate for cancers is less than 1%. This does not mean that one ignores it altogether; just that visible haematuria is a more ominous symptom.
Vegetables like beetroot can discolour the urine (beeturia) enough for somebody to get concerned, but this is a benign phenomenon. Similarly, certain medications can cause discoloration of urine and is not cause for concern.
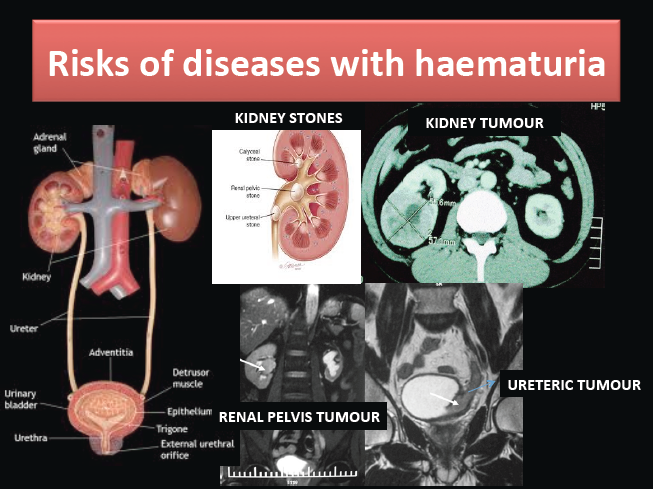
The source of blood can be anywhere along the urinary tract – the upper urinary tract comprising kidneys and ureter, and the lower urinary tract made up by bladder, prostate (in men) and urethra. And it can be due to benign causes like infection or stones. The majority of cancers identified following investigation of haematuria, arise from the lower urinary tract.
The risk of detecting an abnormality following investigation of visible haematuria is similar in both sexes. Although the patient profile described above is classical, no age is exempt from disease. However, in persons with micro-haematuria, the chance of finding serious disease in somebody under the age of 40 is low; international guidelines suggest appropriate discussion between the patient and physician before undertaking invasive investigations in this group of patients.
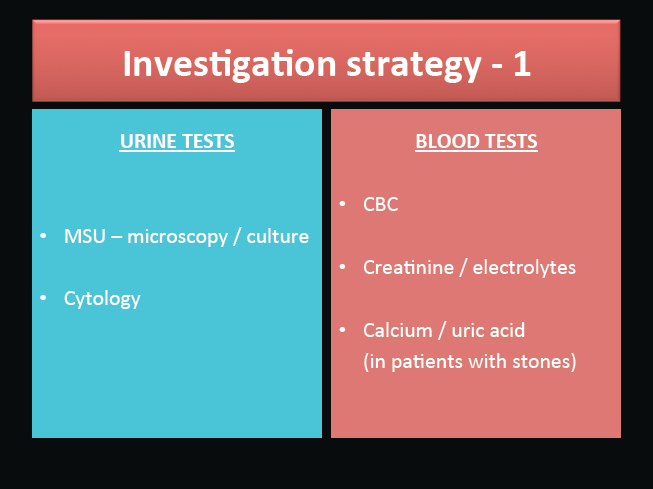
Haematuria is usually a self-limiting symptom, but may occasionally require admission to hospital. This is usually because, it hasn’t settled at all, or making the patient weak (due to significant loss of blood) or unable to void (urinary retention). The duration of the symptom has no bearing to the seriousness of the underlying disease; however brief the symptom may have been, one can still harbour significant underlying disease. Also, identification of infection does not rule out underlying malignant disease. Investigations for haematuria need to undertaken once the infection has been adequately treated.
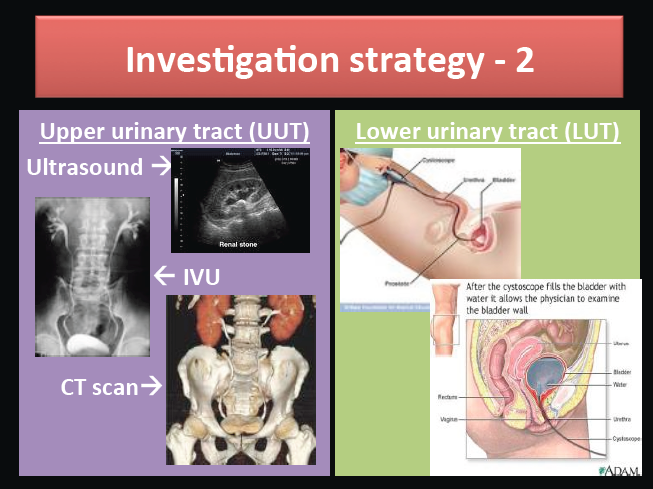
Thanks to modern technology, we are today able to diagnose nearly 100% of those with any identifiable pathology. The upper urinary tract (kidneys / ureter) can be visualised by imaging (ultrasound, intravenous urogram or CT scan) and the lower urinary tract lends itself easily for visual inspection in both the sexes (flexible cystoscopy – inspection of the urethra and bladder with a patient friendly small calibre flexible endoscope).
The latter procedure can be done quite easily in the outpatient setting under local anaesthetic and takes only a few minutes at most (see CYSTOSCOPY – pt guide) . In most centres of excellence, investigation of haematuria is done in fast track clinics and a diagnosis is achieved in the majority within the day. Treatment can then be planned according to the diagnosis, including all urinary tract cancers.

Haematuria is a significant symptom / sign with the possibility of serious underlying disease. Mr Sharma did the right thing by seeing his doctor. If you have had haematuria or are concerned otherwise, why not pay a visit to your GP or your urologist.